




government

Illustration by Jennifer Wenger / AMNews staff
Who are the chronically costly? Health care's 1%
■ The costliest 1% of patients consume one-fifth of all health care spending in the U.S., according to federal data. Health systems are trying to reduce the imbalance.
- WITH THIS STORY:
- » Whose care costs the most?
- » Related content
They are older patients with cancer, diabetes, heart disease and other serious chronic conditions. Many have multiple health problems, and their relatives might not be helping with their care. Most have private insurance, are white and female.
They are the costliest 1% of patients in the U.S. Caring for them accounts for more than 20% of what the nation spends on all of its health care. In contrast, the least costly half of all patients are associated with only 3% of total health spending, according to an Agency for Healthcare Research and Quality analysis of spending data from 2008 and 2009 released in January.
An individual in the costliest bracket typically receives much of his or her care in hospitals -- sometimes in multiple hospitals in the same city. Lack of care coordination is a significant driver of this spending. These missed connections are "probably the primary reason why we cannot manage costs on people who have multiple morbidities," said Ira Klein, MD, chief of staff to the chief medical officer at the insurer Aetna.
Given the stark cost imbalance, health systems, health insurers, federal agencies and state governments are paying an increasing amount of attention to these patients. Care coordination and quality improvement are part of the Obama administration's strategy for limiting the growth of national health spending. But experience has shown that those goals will not be attained easily.
Analyzing the costliest demographic
Hospitals provide a significant amount of care to the costliest 1% of patients. Inpatient care takes up three-fifths of health spending on these patients, according to the AHRQ report. That's twice the rate of the overall population, and the figure does not even include people in nursing homes or other institutional facilities.
The costliest patients, about eight out of 10 of whom are 45 or older, also use more end-of-life care than the general population, said Steven B. Cohen, PhD, author of the AHRQ brief and director of the agency's Center for Financing, Access and Cost Trends. Fewer than 1% of all people died in 2009, but the mortality rate that year for the costliest demographic was nearly 9%.
Private health insurance was the main source of coverage for roughly two-thirds of the costliest patients. Nearly all of the remainder had public coverage, and uninsured patients represented only a few percentage points, according to the report.
Patients' health status has a big influence on where they landed on the cost scale. "People with three or more chronic conditions are usually in that top 10%," said Linda Dunbar, RN, PhD, vice president of care management at Johns Hopkins HealthCare, speaking about Hopkins' Medicaid plan. The plan has approximately 200,000 members.
Untreated mental illness also is a frequent problem for high-cost patients. Mentally ill patients often have difficulty managing their health conditions, said Michael Albert, MD, medical director for internal medicine at the East Baltimore Medical Center, part of the Johns Hopkins system. "Failure of self-management skills is the biggest issue we see."
Dr. Klein said Aetna's costliest groups of services are for care related to cardiac illnesses, cancer, orthopedic problems and women's health, including pregnancy, delivery and care of newborns.
However, Cohen noted, the report does not examine the value of the care provided to the costliest patients, so one shouldn't assume that resources used on high-cost patients have been wasted. Examining patient outcomes is necessary to get a sense of the real benefits of this care, he said.
Staying connected to patients
Increasing the coordination of care is not easy, but many health systems have made headway. Two examples are Geisinger Health System's medical home program and Johns Hopkins' system to predict health care needs.
Geisinger Health System of Pennsylvania uses medical homes and electronic medical records to improve care quality and limit duplication of services. It is a network of physicians, hospitals and a nonprofit health plan with about 270,000 members spanning 44 mostly rural Pennsylvania counties.
Geisinger Health Plan's sickest patients -- those with heart failure, pulmonary disease, diabetes and other conditions -- are enrolled in its patient-centered medical home program called Proven Health Navigator, said Thomas Graf, MD, Geisinger Health System's associate chief medical officer for population health.
Proven Health Navigator patients in active case management maintain close contact with their case managers, who are registered nurses. The RNs examine patients' medical and social support needs and maintain close phone contact. Some heart failure patients have remote monitoring in their homes. The machines allow them to send their weights, prescribed medications and dosages, and symptoms such as shortness of breath to their primary care teams electronically.
Dr. Graf said the medical home program is reducing Geisinger's costs by at least $1.20 for every dollar invested, in part through decreased hospitalizations. "You don't have to avoid a lot of hospitalizations to pay for these management techniques," he said.
Medicaid enrollees represent a minority of the costliest patients, according to the AHRQ report. But the most expensive Medicaid patients also tend to have multiple health problems and the least coordinated care, said Dunbar, of Johns Hopkins.
A decade ago, Johns Hopkins created a program to predict which of their Medicaid health plan members have the highest risks of serious illnesses, Dunbar said. The program places patients into one of five categories based on health status, social and family support, usage of health care and other variables.
"You start to treat the people differently then," Dunbar said. For example, instead of waiting for high-risk patients to get sick, Johns Hopkins case managers remind these patients about recommended medical visits and arrange transportation to appointments, she said. Medium-risk patients receive lifestyle counseling, such as smoking cessation and weight loss support. She said the program has limited annual spending growth for Johns Hopkins' Medicaid plan members to 1% at a time when the national growth average has been closer to 7%.
Dual eligibles a particular problem
But Medicaid enrollees who also are eligible for Medicare are not in the risk management program, Dunbar said. Johns Hopkins and Maryland's Medicaid agency have not yet been able to develop a care management program for these so-called dual eligibles, many of whom consume very high amounts of health spending.
Integrating Medicare and Medicaid is complicated. Medicare has its own systems for risk adjustment, grievances and appeals, and open enrollment, said Charles Milligan, MPH, deputy secretary for health care financing at the Maryland Dept. of Health and Mental Hygiene, the state's Medicaid agency.
"None of those [Medicare standards] cleanly align with state Medicaid programs," Milligan said. Also, Medicare is more focused on treatment of acute health conditions, but Medicaid is more focused on long-term services and support.
State grants in the health reform law are supporting care coordination innovations for dual eligibles. A challenge that faced states applying for these grants was a lack of data on the Medicare services these beneficiaries receive. But the Centers for Medicare & Medicaid Services has helped states fill this knowledge gap, said Melanie Bella, director of the Medicare-Medicaid Coordination Office at the CMS Center for Medicare and Medicaid Innovation. The innovation center plans to use its demonstration authority to test payment models that could reduce or eliminate the incentives for cost-shifting between Medicare and Medicaid.
Persistent health system gaps
Even such innovators as Geisinger and Johns Hopkins can't coordinate health care for all of their costliest patients.
Geisinger Health System operates in areas that are near non-Geisinger physicians and hospitals. The system's ability to share patient care information with these out-of-network doctors and hospitals varies, said Melody Danko-Holsomback, RN, a Geisinger case manager. She and other Geisinger staff are working to improve these connections.
Geisinger health plan members sometimes fall between the cracks. One 57-year-old man with lung cancer who had a non-network primary care doctor visited emergency departments 41 times in a year without being admitted. He was admitted during an additional nine visits, only one of which was planned. He also saw a variety of specialists, but none of the physicians was aware of the scope of services the man received.
Danko-Holsomback said Geisinger is using the example as a case study to improve care for its seriously ill patients.
Patients themselves also have roles to play in preventing costly care, said American Medical Association President Peter W. Carmel, MD. "More than 75% of the nation's health care spending is for the treatment of chronic, often preventable conditions that can be avoided by making healthier lifestyle choices," he said. "Physicians can help the nation get the most for our health care dollar by addressing lifestyle behaviors to reduce the prevalence of chronic disease in patients, and by leading new health care delivery models that improve care coordination while reducing costs."
Dr. Albert said sometimes the level of family involvement in a patient's care is the difference between a frequent hospital visitor and a person who stays healthy. One of his patients, an 85-year-old widower, has congestive heart failure, hypertension and diabetes. The man ends up in hospitals regularly in part because he has difficulty adhering to his medication regimen. He has relatives nearby, but they are not closely involved in his care.
But another patient of Dr. Albert's -- a man with similar health problems -- stayed out of hospitals for three years in a row before he died at the age of 90. The extended run was possible because the man's wife doggedly tracked his medications and health care needs and monitored his diet.
"We called her his little pharmacist, his little nurse," Dr. Albert said.
ADDITIONAL INFORMATION
Whose care costs the most?
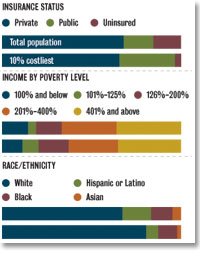
Click to see data in PDF.
Many or most of the patients with the highest health care costs in the nation have health insurance and higher relative incomes, and are white.
| Patient group | All patients | 10% costliest |
|---|---|---|
| Private health insurance | 67.9% | 65.5% |
| Public coverage only | 16.6% | 31.0% |
| Uninsured | 15.5% | 3.6% |
| 100% of poverty and below | 14.4% | 11.3% |
| 101% to 125% of poverty | 4.6% | 9.0% |
| 126% to 200% of poverty | 14.2% | 16.8% |
| 201% to 400% of poverty | 30.7% | 27.7% |
| 401% of poverty and above | 36.2% | 35.2% |
| White | 67.2% | 80.5% |
| Hispanic or Latino | 16.0% | 6.7% |
| Black | 12.0% | 10.6% |
| Asian | 4.8% | 2.2% |
Source: "The Concentration and Persistence in the Level of Health Expenditures over Time: Estimates for the U.S. Population, 2008-2009," Agency for HealthCare Research and Quality, January (link)







